
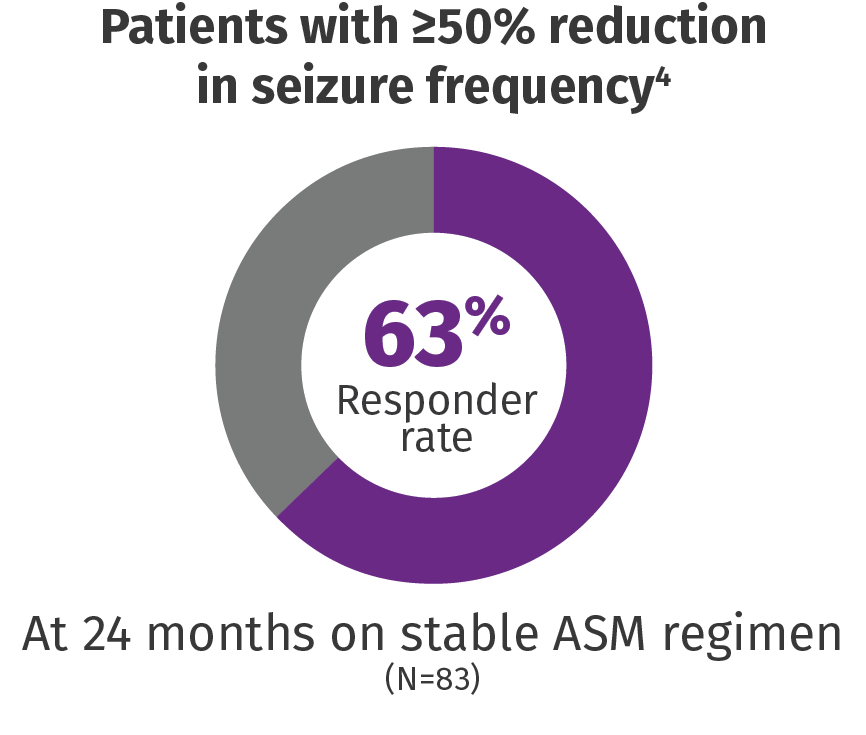
VNS Therapy™ reduces the frequency, duration, and severity of seizures and improves postictal recovery
In a study of 347 pediatric patients followed up for 24 months2:
.jpg?language=en-US)
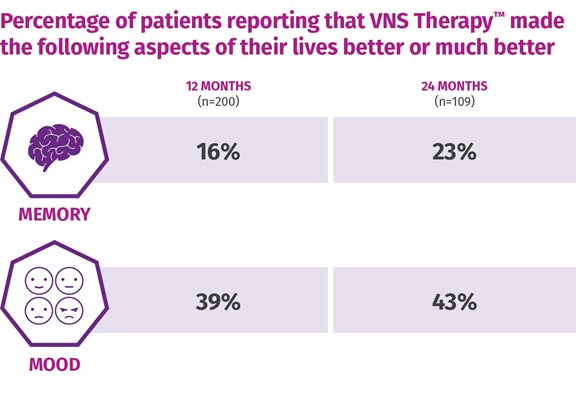
One-third of patients were considered "much improved" or "very much improved" following 12 months of adjunctive VNS TherapyTM (n=78), with sustained and improved scores continuing up to 24 months.5
Based on the clinican's assessment of the patient's overall condition (CGI-I).
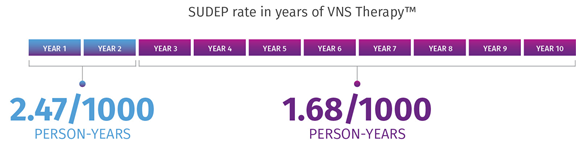
VNS Therapy may be associated with lower SUDEP rates.6
In a retrospective claims analysis, age-adjusted SUDEP rates decreased over time from years 1 to 2 (2.47/1000 person-years) to years 3 to 10 (1.68/1000 person-years).* A study on 277,661 person-years of up to 10 years of follow-up and 3689 deaths, including 632 cases of SUDEP, showed that long-term VNS Therapy is associated with lower SUDEP rates. The data suggest that SUDEP risk decreases during long-term follow-up of patients with refractory epilepsy receiving VNS Therapy.
*Limitations: This finding might reflect several factors, including ASM use, lack of a control group/seizure baseline, the natural long-term dynamic of SUDEP rate, attrition, and the impact of VNS Therapy. The role of each of these factors cannot be confirmed due to the limitations of study.
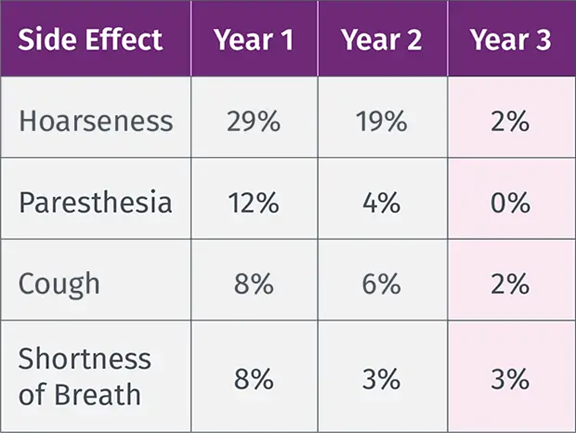
VNS TherapyTM Safety Profile

